Creatine
Creatine is one of the most popular sports supplements currently available, but creatine itself is not a new thing. Creatine is an essential component of skeletal muscle which was initially discovered in the early 1800’s and named after the Greek word ‘Kreas’ meaning ‘muscle’. In 1847, a researcher by the name of Leibig hypothesised that creatine was a necessary metabolite in skeletal muscle activity after he noticed that wild foxes stored 10 times more creatine in their muscle cells compared to relatively inactive captive-bred foxes. Since the 1990’s a rapid increase in research has made it one of the most well-understood things we will talk about in this module.
Creatine is stored primarily within muscle tissue, with around 95% of stored creatine being found here, mostly in the form ‘phosphocreatine’ which is simply creatine with an added phosphate group (the rest is stored as free creatine). The remaining 5% is stored mostly in the brain and testes. Although this small amount of non-muscular creatine storage may seem insignificant, it is incredibly important.
A rare genetic defect carried on the X (male) chromosome causes an impairment of the creatine transporter (a specific cellular protein responsible for transporting creatine into a cell). This defect results in an almost complete absence of creatine in the brain, which seems to lead to severe in severe speech and language delays, epilepsy and autism spectrum behaviour.
The role of creatine in exercise is in relation to the energy systems that were discussed in module 2. ATP is hydrolysed to release the energy needed to allow muscles to contract the energy needed for you to move. This ATP is quickly depleted meaning that it must be replenished via aerobic or anaerobic pathways.
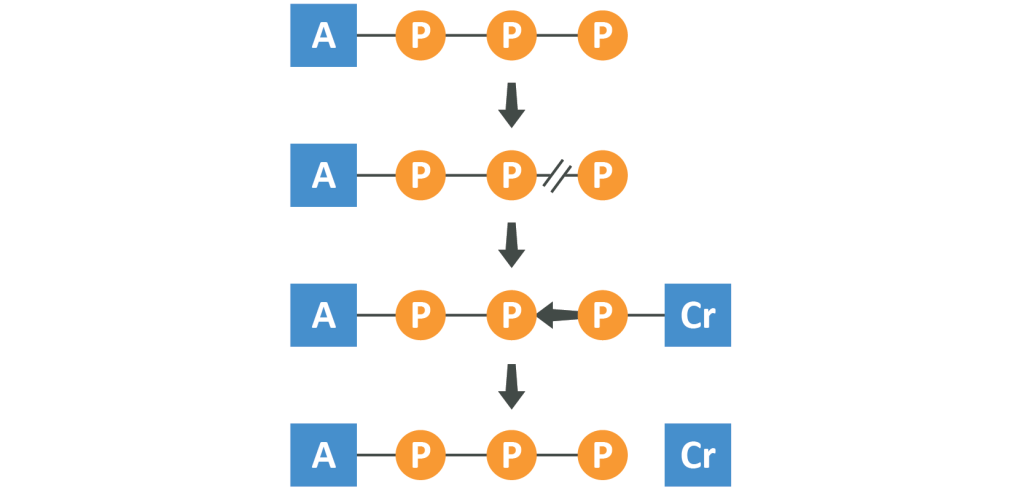
These pathways are, however, not able to produce re-usable ATP for exertions lasting around 5-10 seconds. In order to keep a usable supply we need to tap in to the ATP/PhosphoCreatine system which uses molecules of creatine stored in muscle cells alongside a phosphate group as a ‘phosphate doner’, in the following three step fashion:
- ATP is hydrolysed to ADP to release energy
- Phosphocreatine stored in the muscles interacts with the enzyme
- creatine kinase, in turn losing its stored phosphate group
- ATP synthase then attaches that free phosphate to the newly made ADP, leaving usable ATP
This process does not use oxygen and occurs extremely rapidly meaning that for a sub 100 metre sprint, set of heavy lifts, jump, kick, punch or other explosive work, the energy can be made available without the use of glucose or fatty acids.
The average 70kg human body contains around 120g of creatine of which 2g is turned over in the average day, meaning that it’s broken down (to creatinine, which is then excreted) and then replaced. The replacement creatine can be attained via the diet in meats and fish, though the content of these foods is low, or synthesised endogenously by the fusing together or glycine, arginine and methionine. This process ensures that creatine is always available when needed, but diets low in exogenous creatine (vegetarian or vegan diets especially) tend to leave individuals with lower than average creatine stores.
Supplementation of creatine can increase the storage potential of creatine for omnivorous individuals by 10-20% and for vegetarian and vegans by up to 40%, meaning that the above process of ATP recycling using the ATP/PC energy system becomes far more efficient, leading to a number of benefits, primarily due either to improved performance ability or due to the adaptations caused by improved performance. Short-term supplementation appears to improve:
- Maximal power/strength by 5-15%, useful for most explosive endeavours
- Work capacity at maximal effort in resistance and sprint training by 5-15%, meaning that you are able to repeat a maximal performance bout for a greater number of rounds during a given session – useful for resistance training, interval training or team sports, amongst others
- Improved performance in single effort sprint training by 1-5%
This has been tested using cycling power, bench press and jump squat work capacity and sprint, soccer and swimming performance. And then longer term, supplementation seems to improve general training quality, resulting in a 5-15% increase in strength and performance. Some physiological effects expected from creatine supplementation include increased lean body mass, strength, sprint performance, power, rate of force development and muscle size.
As mentioned, most of these effects occur not because of the direct impact of creatine itself but because creatine allows you to train longer and harder, meaning that you are able to create a greater training stimulus leading to a heightened amount of adaptation. With that said, some of the lean body mass gained from creatine supplementation is likely to occur due to water weight gain. If an individual follows a loading protocol (described below) then a gain of 1-2kg in the first 2 weeks is considered normal, with the majority of this being water.
Creatine is considered safe with no proven side effects, though it must be said that very long-term research has yet to be done and so it cannot be said conclusively that no harmful effects would come of continuous use for decades. It is unlikely, however, as short-term studies have not shown damage to the kidneys (the most logical place for harm, due to filtration) in over 5 years of use. Additionally, creatine is being explored for clinical use in the treatment/ management of brain injuries, spinal cord injuries, muscular dystrophy, diabetes, blood lipid markers and pulmonary disease, leading us to consider creatine more than likely to be perfectly safe. The only notable exception to this is children and adolescents – due to the lack of concrete evidence it is unwise to recommend creatine supplementation to those under the age of 16.
Though numerous creatine isomers are available, there is no robust evidence to date to show that more expensive forms have better efficacy than the comparatively cheap form Creatine Monohydrate. Creatine monohydrate seems to be able to maximally impact muscle stores of phosphocreatine over time, and so this is the form most often recommended. Combining creatine with other supplements does not appear to improve its efficacy, with one notable exception. Combining creatine with beta alanine appears to increase the overall effect on strength, lean mass and bodyfat percentage in addition to the benefits of adding beta alanine per se. The only other thing so far shown to improve the effectiveness of creatine is carbohydrate. Adding 93g of carbohydrates, or 47g of carbohydrate and 50g of protein have both been shown to improve the muscular uptake of creatine by around 60%. This has not yet been shown to translate to improving the actual results desired (performance, body composition), but is worth considering. You could also take it alongside meals.
The dosage for creatine monohydrate is around 3-6g per day, every day. This could be taken post-workout alongside a higher carbohydrate meal or post-workout shake to take advantage of the above theoretical benefits, though this is not likely to be critical. Prior to this, a loading protocol is often used which consists of consuming 0.3g of creatine per day per kg of bodyweight for 5-7 days, split into 3-4 doses. For a 70kg individual this would equate to 4 doses of 5g every day for the first 5-7 days followed by a maintenance dose of 3-5g per day.
Note: The loading protocol isn’t needed, but it is effective at increasing muscle creatine saturation levels to the highest levels to which they will go, meaning you benefit from supplementation much more quickly.